Anisometropia
Anisometropia is the condition in which the two eyes have unequal refractive (glasses) power. The name is derived from Greek components: an- "not," iso- "same," metr- "measure," opia "eye" or "sight". Often each eye is nearsighted (myopia) or farsighted (hyperopia), and then to meet the technical criteria of anisometropia the difference between the right and left eye is two or more diopters (the inverse of a meter, which is how an optical lens power is described). Although much less common, it is possible to have one nearsighted and one farsighted eye - this is a unique subset of anisometropia called antimetropia. Anisometropia is actually fairly common. An estimated 20% of people have an inter-ocular difference of 0.5D or greater, and 2-3% have a difference of 3D or more.
What's Concerning About Anisometropia?
In brief, anisometropia is one of the causes of amblyopia (lazy eye). Anisometropia that is uncorrected leaves the visual system in conflict - one eye is likely blurrier than the other. The result is the brain focuses on the least-blurry image. If the amount of anisometropia is large and is not corrected, the patient's visual system (the visual portion of the thalamus, visual cortex, and other processing parts of the brain) may not develop correctly. The result is the brain subconsciously ignores vision from one eye and fails to learn to use both eyes together. This is called suppression. If a patient suppresses, normal binocular vision is disrupted, which can result in amblyopia.
Types of Anisometropia
Simple Anisometropia
Simple anisometropia occurs when only one eye has a refractive error. The eye can be either hyperopic (farsighted) or myopic (nearsighted). Simple anisometropia causes one eye to see a blurry image while the other eye sees a clear image.
Compound Anisometropia
Compound anisometropia occurs when both eyes are either hyperopic (farsighted) or myopic (nearsighted), however, there is still a significant difference in the refractive errors of the two eyes. This form of anisometropia causes both eyes to see blurry images, but one eye’s vision will be significantly blurrier.
Antimetropia (Mixed Anisometropia)
Antimetropia (sometimes called mixed anisometropia) occurs when both eyes have refractive errors but one is myopic (nearsighted), and the other is hyperopic (farsighted).
Meridional Anisometropia
This form of anisometropia is caused by high astigmatism (also called cylinder) correction in one eye. This means the refractive error correction is worse along one meridian or axis, and the eyes have astigmatism of different magnitudes.
Other Cause of Anisometropia
Aphakia
Aphakia occurs with the lens of the eye (the focusing mechanism) is removed and not replaced with an artificial lens (this is called pseudophakia if an artificial intraocular lens is implanted). Aphakia may be intentional (for example with a baby that has a dense cataract). The resulting difference in glasses correction may be quite large as the lens of the eye contributes a refractive power of about +16 diopters.
Signs and Symptoms of Anisometropia
Generally speaking, with anisometropia, one sees a blurrier image with one eye compared to the other. The patient may also notice a smaller image in one eye and a larger image in the other eye. Anisometropia can also result in diplopia (double vision). Some symptoms may include:
- Eyestrain
- Poor depth perception
- Headaches
- Nausea
- Light sensitivity
- Tiredness
- Dizziness
Though anisometropia can be present from birth, it is not typically diagnosed until a childhood eye examination. Children who have anisometropia may not show any symptoms. For the very young, parents should note any preferential looking, an eye turn, or failure to reach developmental milestones, especially with mobility. Children may also complain of blurry vision or headaches. Ideally, all children should have a comprehensive vision exam by an optometrist or ophthalmologist during the first year of life to help identify this condition and others. The InfantSEE program was created to help encourage early eye exams in children to catch conditions such as anisometropia.
Treatment for Anisometropia
Treatment for anisometropia primarily involves correcting the refractive difference between the eyes. This is often done with a pair of eyeglasses. Due to the risk of amblyopia, it is not uncommon for an eye doctor to prescribe a pair of lenses and then see the patient back in one or two months for a re-evaluation.
More severe cases of anisometropia may not respond as well to glasses. This is primarily due to an optical principle called aniseikonia (an-ice-eh-cone-e-a). This is partially due to the anisometropia, and partially due to the attempt to correct it. Lenses in general either concave or convex - a minification lens or magnification lens, respectively (we'll use the term "magnification" going forward). If the magnification between the two eyes is too unequal, a patient may be unable to fuse the images and may complain of the same symptoms previously described (eye strain, headache, dizziness, etc.).
For our image below, the screen is out "window to the brain" and shows what the brain sees.
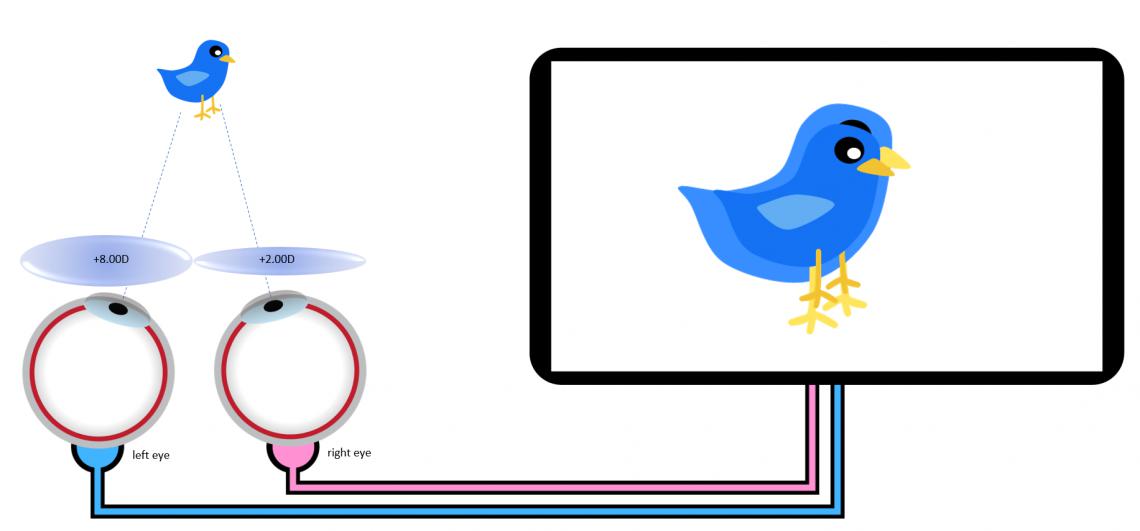
This is a simplified example of anisometropia where the left eye is corrected with a +8.00D lens and the right is corrected with a +2.00D lens. A little optics calculation (which is beyond the scope of this article but takes into account the power of the lenses, curve of the lenses, thickness of the lenses, material of the lenses, and distance of the lenses from the eye) calculates out to about 14% magnification left eye and about 3.5% magnification right eye.
So why is this an issue? Well, as you see by the above image, this magnification difference between the two eyes results in one image being larger than the other, which is very difficult for the brain to match together to make a single image. In fact, the brain can only tolerate a mismatch of about 6%, which is about 3 diopters of difference between the right and left eye correction.
Fortunately, the simple way to equalize the magnification difference between lenses is to place the lens directly on the eye - a contact lens. Even very young children (even babies!) may be prescribed a contact lens correction to reduce the risk of developing amblyopia (lazy eye).
Additionally, if anisometropia has caused amblyopia, then treatment may include traditional vision rehabilition for amblyopia, such as vision therapy, patching, or eye drops.
References:
The Relationship between Anisometropia and Amblyopia (https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3773531/)
Refractive Errors (https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5143802/)
Care of the Patient with Amblyopia (https://www.aoa.org/documents/optometrists/CPG-4.pdf)
The Vision Wiki
- Lazy Eye
- History of Lazy Eye
- Convergence Disorders
- Convergence Insufficiency
- Exophoria
- Esophoria
- Medical Terms
- Accommodation Disorders
- Accommodative Esotropia
- Accommodative Insufficiency
- Amblyopia
- Lazy Eye in Adults
- Strabismic Amblyopia
- Refractive Amblyopia
- Anisometropia
- Critical Period
- Strabismus
- Anomalous Retinal Correspondence
- Transient Strabismus
- Exotropia
- Esotropia
- Hypotropia
- Hypertropia
- Eye Problems
- Binocular Vision
- Physiology of Vision
- Lazy Eye Treatments
- Reading
- Fields of Study
- Research
- Glaucoma
- Virtual Reality
- Organizations